The information highlighted (if any) are the most recent updates for this brand.
Trimetazidine dihydrochloride.
One prolonged-release hard capsule contains 80 mg of trimetazidine dihydrochloride.
Excipient with known effect: Sucrose 33.75mg per capsule.
Excipients/Inactive Ingredients: Capsule content: Sugar sphere containing sucrose and maize starch, Hypromellose, Ethylcellulose, Tributyl acetylcitrate, Talc, Magnesium stearate.
Capsule shell: Gelatin, Titanium dioxide (E171), Red iron oxide (E172).
Printing Ink: Shellac Glaze-45% in Ethanol, Titanium dioxide (E171), Simethicone, Propylene Glycol (E1520), Ammonium hydroxide 28% (E527).
Pharmacotherapeutic group: Other cardiovascular antianginal drug. ATC code: C01EB15.
Pharmacology: Pharmacodynamics: Mechanism of action: By preserving energy metabolism in cells exposed to hypoxia or ischaemia, trimetazidine prevents a decrease in intracellular ATP levels, thereby ensuring the proper functioning of ionic pumps and transmembrane sodium-potassium flow whilst maintaining cellular homeostasis.
Trimetazidine inhibits β-oxidation of fatty acids by blocking long-chain 3-ketoacyl-CoA thiolase, which enhances glucose oxidation. In an ischaemic cell, energy obtained during glucose oxidation requires less oxygen consumption than in the β-oxidation process. Potentiation of glucose oxidation optimizes cellular energy processes, thereby maintaining proper energy metabolism during ischaemia.
Pharmacodynamic effects: In patients with ischaemic heart disease, trimetazidine acts as a metabolic agent, preserving the myocardial high-energy phosphate intracellular levels. Anti-ischemic effects are achieved without concomitant haemodynamic effects.
Clinical efficacy and safety: Clinical studies on trimetazidine have demonstrated its efficacy and safety in the treatment of patients with chronic angina, either alone or when the benefit from other antianginal medicinal products was insufficient.
In a 426-patients randomized, double blind, placebo-controlled study (TRIMPOL-II), trimetazidine (60mg/day) added to metoprolol 100mg daily (50 mg b.i.d) for 12 weeks significantly improved statistically exercise tests parameters and clinical symptoms as compared to placebo: total exercise duration +20.1s, p= 0.023, total workload +0.54 METs, p=0.001, time to 1-mm ST-segment depression +33.4s, p=0.003, time to onset of angina +33.9s, p<0.001, angina attacks/week -0.73, p=0.014 and short acting nitrates consumption/week, -0.63, p=0.032, without hemodynamic changes.
In a 223 patients randomized, double blind, placebo-controlled study (Sellier), one 35 mg trimetazidine modified release tablet (b.i.d.) added to 50 mg atenolol (o.d.) for 8 weeks produced a significant increase (+34.4s, p=0.03) in the time to 1-mm ST-segment depression in exercise tests, in a sub-group of patients (n=173), when compared to placebo, 12 hours after taking the drug. A significant difference was also evidenced for the time to onset of angina pectoris (p=0.049). No significant difference between groups could be found for the other secondary endpoints (total exercise duration, total workload and clinical endpoints).
In a 1962 patients three-month randomised, double-blinded study (Vasco study) on top of atenolol 50 mg/d, two dosages of trimetazidine (70 mg/d and 140 mg/d) were tested versus placebo. In the overall population, including both asymptomatic and symptomatic patients, trimetazidine failed to demonstrate a benefit on both ergometric (total exercise duration, time to onset of 1mm ST and time to onset angina) and clinical endpoints. However, in the subgroup of symptomatic patients (n= 1574) trimetazidine (140 mg) significantly improved total exercise duration (+23.8 s versus +13.1 s placebo; p=0.001) and time to onset of angina (+46.3 s versus +32.5 s placebo; p=0.005).
In a 165 patients three-month randomised, double-blind acceptability study on top of both routine antianginal therapies and secondary prevention therapy, the safety profile of trimetazidine 80 mg once daily was shown to be similar to that of trimetazidine MR 35 mg bid. No unexpected adverse event was reported and the study showed no concern regarding the once daily intake of trimetazidine 80 mg.
Pharmacokinetics: Absorption: After oral administration of trimetazidine 80mg capsule, trimetazidine PK profile is flat with a peak of trimetazidine concentration reached around 14 hours after drug intake. Over dosing interval i.e. 24 hours the plasma concentration remains for 15 hours at levels above or equal to 75% of the maximum concentration. Steady state is reached by the third dose intake (3 days).
Food intake has no effect on trimetazidine PK after administration of the 80mg formulation.
Distribution: The volume of distribution is 4.8 l/kg; protein binding is low (16%).
Elimination: Trimetazidine is primarily eliminated in the urine, mainly as unchanged form. The elimination half-life is on average 7 hours in healthy young volunteers and 12 hours in elderly (more than 65 years).
Total clearance of trimetazidine mainly consists of renal clearance which is directly correlated to creatinine clearance and, to a lesser extent, of liver clearance which is reduced with age.
Special populations: Elderly: The elderly may have increased trimetazidine exposure due to age-related decrease in renal function. A dedicated pharmacokinetic study performed in elderly 75-84 years or very elderly (≥85years) participants showed that moderate renal impairment (creatinine clearance between 30 and 60 ml/min) increased respectively by 1.0 and 1.3 fold the Trimetazidine exposure in comparison to younger participants (30-65 years) with moderate renal impairment.
A specific clinical study carried out in an elderly population (older than 75 years old) using a dosage of 2 tablets of trimetazidine MR 35mg per day taken in 2 doses, analysed by a kinetic population method, showed on average a 2-fold increase in plasma exposure in patients with severe renal impairment (creatinine clearance below 30ml/min) as compared to those with a creatinine clearance above 60 ml/min.
No safety concern was observed in the elderly population as compared to the general population.
Renal impairment: Trimetazidine exposure is increased on average by 1.7-fold in patients with moderate renal impairment (creatinine clearance between 30 and 60 ml/min), and on average by 3.1-fold in patients with severe renal impairment (creatinine clearance below 30ml/min) as compared to healthy volunteers, with normal renal function.
No safety concern was observed in this population as compared to the general population.
Paediatrics: The pharmacokinetics of trimetazidine has not been studied in the paediatric population (<18 years old).
Toxicology: Preclinical safety data: Chronic toxicity studies conducted by the oral route in dogs (5 to 40 mg.kg-1.d-1) and rats (5 to 200 mg.kg-1.d-1), showed a good safety profile.
Neither embryo-foetotoxic effect nor teratogenicity were detected in mice and in rabbits. A general study on reproduction and embryogenesis in 3 generations of rats showed no anomalies.
The genotoxic potential was thoroughly assessed with in vitro studies including the evaluation of the mutagenic and clastogenic potential and one in vivo study. All tests were negative.
Trimetazidine is indicated in adults as add-on therapy for the symptomatic treatment of patients with stable angina pectoris who are inadequately controlled by or intolerant to first-line antianginal therapies.
Posology: The dose is one capsule of 80mg of trimetazidine once daily during breakfast.
The benefit of the treatment should be assessed after three months and trimetazidine should be discontinued if there is no treatment response.
Special populations: Patients with renal impairment: In patients with moderate renal impairment (creatinine clearance [30-60] ml/min) (see Precautions and Pharmacology: Pharmacokinetics under Actions), the recommended dose is reduced by half ie, 1 tablet of 20mg twice daily, one in the morning and one in the evening during meals or 1 tablet of 35mg in the morning during breakfast.
Elderly patients: Elderly patients may have increased trimetazidine exposure due to age-related decrease in renal function (see Pharmacology: Pharmacokinetics under Actions). In patients with moderate renal impairment (creatinine clearance [30-60] ml/min), the recommended dose is reduced by half ie, 1 tablet of 20mg twice daily, one in the morning and one in the evening during meals or 1 tablet of 35mg in the morning during breakfast. Dose titration in elderly patients should be exercised with caution (see Precautions).
Paediatric population: The safety and efficacy of trimetazidine in children aged below 18 years have not been established. No data are available.
Method of administration: Capsule must be taken orally without opening it, once daily i.e. one in the morning during breakfast.
Limited information is available on trimetazidine overdose. Treatment should be symptomatic.
Hypersensitivity to the active substance or to any of the excipients listed in Description.
Parkinson disease, Parkinsonian symptoms, tremors, restless leg syndrome and other related movement disorders.
Severe renal impairment (creatinine clearance <30ml/min).
This medicine is not a curative treatment for angina attacks, nor is it indicated as an initial treatment for unstable angina or myocardial infarction, nor in the pre-hospital phase or during the first days of hospitalisation.
In the event of an angina attack, the coronaropathy should be reevaluated and an adaptation of the treatment considered (medicinal treatment and possibly revascularisation).
Trimetazidine can cause or worsen parkinsonian symptoms (tremor, akinesia, hypertonia), which should be regularly investigated, especially in elderly patients. In doubtful cases, patients should be referred to a neurologist for appropriate investigations.
The occurrence of movement disorders such as parkinsonian symptoms, restless leg syndrome, tremors, gait instability should lead to definitive withdrawal of trimetazidine.
These cases have a low incidence and are usually reversible after treatment discontinuation. The majority of the patients recovered within 4 months after trimetazidine withdrawal. If parkinsonian symptoms persist more than 4 months after drug discontinuation, a neurologist opinion should be sought.
Falls may occur, related to gait instability or hypotension, in particular in patients taking antihypertensive treatment (see Adverse Reactions).
Caution should be exercised when prescribing trimetazidine to patients in whom an increased exposure is expected: moderate renal impairment (see Dosage & Administration and Pharmacology: Pharmacokinetics under Actions), elderly patients older than 75 years old (see Dosage & Administration).
This drug contains sucrose. Patients with rare hereditary problems of fructose intolerance, glucose galactose malabsorption or sucrose-isomaltase insufficiency should not take this medicine.
Athletes: This medicinal product contains a drug substance that may give a positive result in anti-doping tests.
Effects on ability to drive and use machines: Trimetazidine does not have haemodynamic effects in clinical studies, however cases of dizziness and drowsiness have been observed in post-marketing experience (see Adverse Reactions), which may affect ability to drive and use machines.
Pregnancy: There are no data from the use of trimetazidine in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity (see Pharmacology: Toxicology: Preclinical safety data under Actions). As a precautionary measure, it is preferable to avoid the use of trimetazidine during pregnancy.
Breastfeeding: It is unknown whether trimetazidine is excreted in human milk. A risk to the newborns/infants cannot be excluded. Trimetazidine should not be used during breast-feeding.
Fertility: Reproductive toxicity studies have shown no effect on fertility in female and male rats (see Pharmacology: Toxicology: Preclinical safety data under Actions).
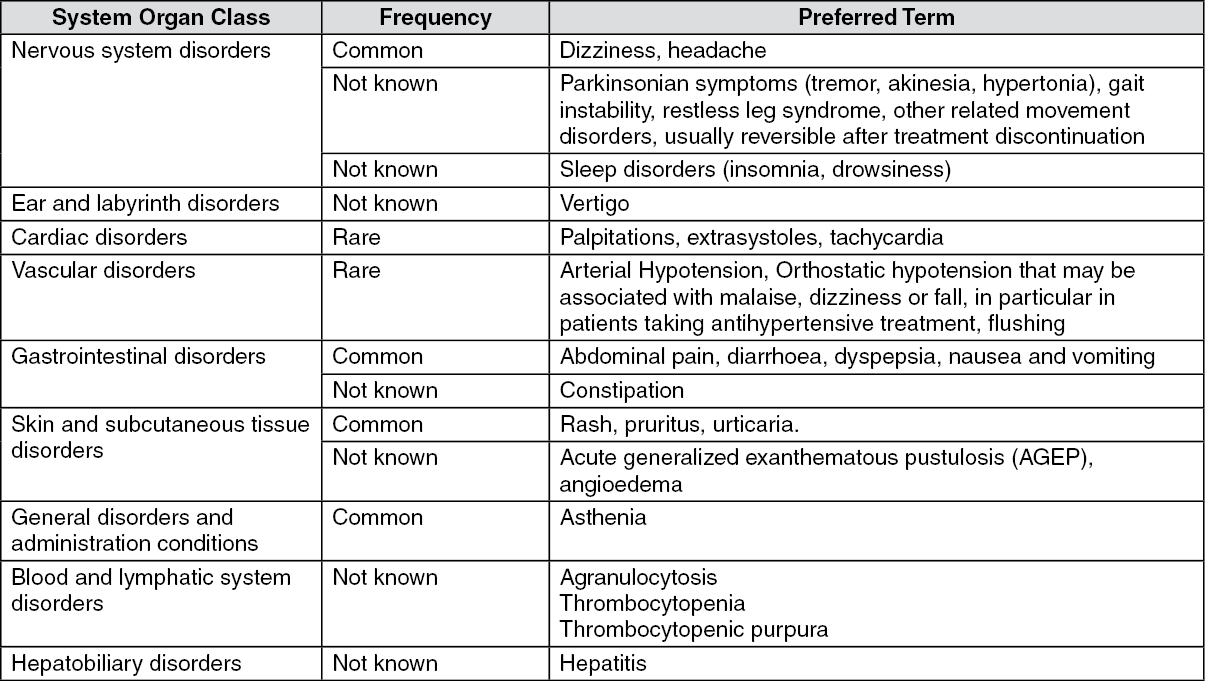
Adverse reactions, defined as adverse events considered at least possibly related to trimetazidine treatment are listed as follows using the following convention frequency: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
No drug interactions have been identified.
Special precautions for disposal: No special requirements for disposal.
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Incompatibilities: Not Applicable.
Store below 30°C.
Shelf life: 36 months.
C01EB15 - trimetazidine ; Belongs to the class of other cardiac preparations.
Vastarel XR PR cap 80 mg
10's;30's





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
